In infants, the individual skull plates must be connected to each other in a mobile manner via the still soft cranial sutures. This is the only way to ensure that the developing and growing brain has sufficient space in the skull. Not all cranial sutures are always affected by craniosynostosis.
The extent of craniosynostosis can also change during growth.
Craniosynostosis can lead to neurological impairments such as
- Reduced intelligence
- visual disturbances
- pain
It also leads to aesthetic symptoms such as
- Asymmetries
- Conspicuous head shapes
- Facial deformities
The ossification of the cranial sutures takes place via a fine interplay between the base of the skull and the meninges with the skull bone. Brain growth sets the pace for the extent and speed of this process.

The large fontanel and the small fontanel are important and generally known points. These are two openings of connective tissue located at the intersection of the cranial sutures.
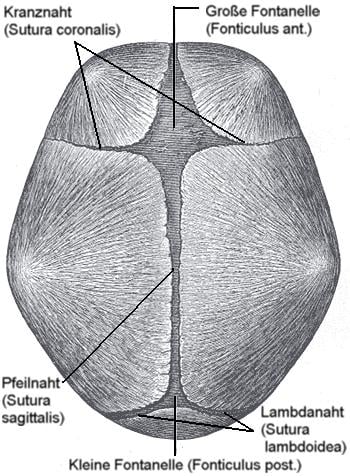
The fontanelles are expansion reserves and can be easily felt on the baby's head. The small fontanel closes at an age of around 2-5 months, the large one at around two years.
In one-year-old babies, 90 percent of brain growth is complete. By the age of two, the cranial sutures have closed and the remaining bone growth is much slower.
Craniosynostosis is the generic term for premature ossification of the skull in fetuses and infants. Certain terms are used depending on the cranial suture affected:
- Frontal suture synostosis
Frontal suture synostosis refers to the ossification of the frontal suture that runs vertically in the forehead. As a result, normal development of the forehead width is not possible. Instead, the result is a spherical forehead, inadequate coverage of the lateral eye sockets and retracted temples.
- Sagittal suture synostosis
Premature ossification of the sagittal suture, which lies between the anterior and posterior fontanel, impairs growth in the width of the vertex. To compensate for this, the forehead and the back of the head bulge forward above average, resulting in a narrow, elongated head.
- Coronal suture synostosis
An asymmetrical forehead occurs when the coronal sutures are affected. These are located on the right and left side of the head in the area of the hairline. Experts also call it anterior plagiocephaly. The affected side is flatter here.
It is also common:
- A significant protrusion of the forehead on the other side
- Changes in the eye socket area, making the eye appear enlarged. Deviations can also occur in the ear area or on the nose.
Asymmetries at the back of the head are usually caused by ossification of one of the two lambdoid sutures at the back of the head. In this type of lambdoid suture synostosis, which usually occurs on one side, the back of the head flattens on one side.
There is a compensatory growth in the reciprocal vertex region. The "posterior plagiocephaly". Due to this asymmetry, the ears usually appear unevenly positioned.
In microcephalus, all cranial sutures are prematurely ossified. The result is an extremely small head shape and severely impaired brain development.
The following symptoms occur:
- The growth disorder of the skull caused by craniosynostosis can be recognized by an asymmetry of the head or face.
- The cranial cavity is too small, which leads to increased intracranial pressure. This means that the growing brain presses against the small and prematurely solidified skull from the inside.
- Damage to the brain, including visual impairment, is a typical consequence.
- Deformities in the facial area are not just an aesthetic problem, but can also lead to functional impairment of the airways.
- In addition, reduced eye sockets can make it difficult to close the eyelids.
Craniosynostosis is often suspected at the sight of the typical changes in head shape. The cranial index gives doctors additional guidance.
X-rays and computer tomography images with three-dimensional representations of the skull conditions confirm the diagnosis. This information helps the doctor to prepare the subsequent therapy.
Additional diagnostic procedures include an EEG to measure the electrical brain waves, further neurological examinations and an ophthalmologic examination.
Only surgical measures can be used to treat craniosynostosis.
Up to the third month of life, doctors can perform an endoscopic operation to remove a limited amount of bone from the ossified cranial suture.
The child then wears a special helmet until the age of 18 months. This ensures that the skull takes on a normal head shape. Between the fifth and 12th month of life, doctors can permanently restore the final uniform head shape during an operation.
 A special helmet helps to bring the child 's skull into a more regular shape @ peter /AdobeStock
A special helmet helps to bring the child 's skull into a more regular shape @ peter /AdobeStock
Doctors usually treat craniosynostosis surgically within the first year of life, as the bone is easier to shape.
In addition, the ability to form new bone decreases considerably. Nevertheless, older children can also be operated on.
These are the most common surgical methods:
Fronto-orbital reshaping is the most frequently performed operation to correct malformations and functional disorders in the forehead area.
Parts of bone are removed, reshaped and reinserted. The supporting plate used consists of resorbable material that gradually dissolves. The delicate scar is well concealed behind the hairline.
- Parieto-occipital reshaping
This surgical method is used to reshape the back of the head, for example in the case of lambdoid synostosis. Several surgical techniques are available for this.
Decompression surgery is used in the cranial region of the hairy head. The surgeon makes radial incisions in the skull bone.
The bone flaps push the growing brain apart. The bone parts later fuse together. Decompression surgery is possible up to the end of the third month of life.
The success of surgical treatment of craniosynostosis is permanent. The healing process is generally good. In most cases, the abnormal shape of the skull can be almost completely eliminated.
The cosmetic results in the facial area are also extremely good.








