Spinal fusion can help to treat or relieve the symptoms of many spinal conditions. While the technique limits flexibility to some extent, this benefits spinal disorders in which movement has become painful. Such disorders may include:
A spinal fusion procedure may also include a discectomy. This entails removing a disc and inserting bone grafts to bridge the empty space. A cervical fusion involves a similar procedure in the neck (cervical spine).
Spinal fusion is used to reduce pain by stabilising your spinal structure and is performed under general anaesthetic. This surgery is usually a lengthy procedure that can last some hours.
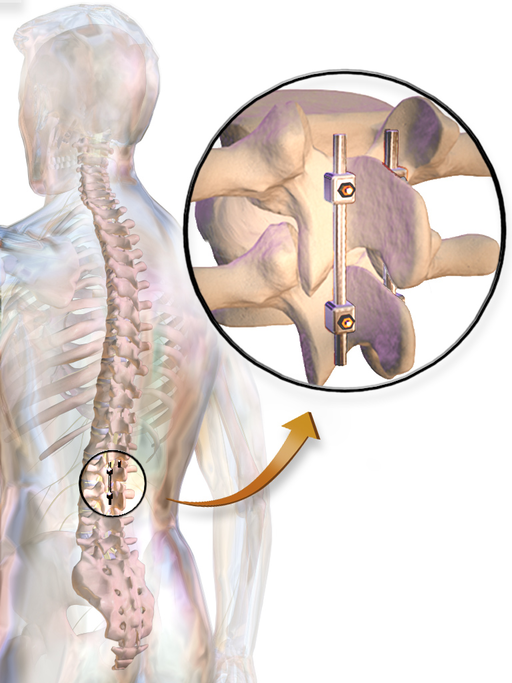
The technique may use your own bone (an autograft), synthetic bone or bone obtained from a bone bank (an allograft), and requires an incision at the spinal area where fusing is to take place. When the bone graft has been successfully installed, it is often supported by screwed metal plates and rods to prevent spinal movement and speed the healing process.
As with any other form of surgery, spinal fusion procedures carry certain risks, such as:
- wound infection
- blood clots
- bleeding and blood loss
- respiratory problems
- the risk of stroke or heart attack during the procedure
- slow and/or unsatisfactory wound healing
- reactions to anaesthetic or medication
Spinal fusion surgery also poses a further risk of developing the following rare complications:
- infection within the wound or treated vertebrae
- spinal nerve damage, which can result in weakness, pain and bladder or bowel problems
- additional stress to the bone structures next to the fused vertebrae
- persistent pain at the location of the bone graft
- blood clotting in the legs (which can be life-threatening if a clot reaches the lungs)
The most dangerous complications are infections and blood clots, which would primarily appear during the early weeks after surgery.
Seek emergency medical help if a blood clot causes any of the following symptoms:
- sudden swelling in a calf, ankle or foot
- any redness or tenderness immediately above or below your knee
- calf pain
- groin pain
- breathlessness
Seek emergency medical help if an infection causes any of the following symptoms:
- redness or swelling around the edge of a wound
- blood, pus or any other liquid leaking from the wound
- fever, chills or high temperature above 38° C / 100° F
- shaking
For those experiencing lower back pain as a result of lumbar degenerative disc disease, the possible alternatives to spinal fusion include:
- angioplasty, or IDET (intradiscal electrothermal coagulation) a procedure that applies heat to the annulus (the fibrous outer core of the disc space). This is a minimally invasive technique, which appears to offer relatively marginal benefits.
- artificial discs present the (theoretical) benefit of preserving spinal motion – unlike spinal fusion, which aims to limit mobility. However, the risk of eventual disc failure, thus prompting a need for further, risky revision surgery has somewhat compromised the potential gains.
- posterior dynamic stabilization seeks to preserve mobility, while also relieving the pressure on a diseased vertebral disc to allow healing to take place. This method is still at the testing stage.
- disc regeneration by biological means is a technique that has been used with some success in the research phase but is not yet at the stage where it can be offered as a viable treatment.







































