The ankle joint (talocrural joint) consists of three bones:
- Tibia (shinbone)
- Fibula
- Talus (ankle bone)
The tibia and fibula form the ankle mortise, which provides the talus with a centered and stable fit. The talocrural joint controls dorsiflexion and plantarflexion of the foot. Within the ankle mortise, the talus performs gliding and slight rotational movements.
The articular surfaces of the tibia, fibula, and talus are covered by a thin but highly elastic layer of cartilage.
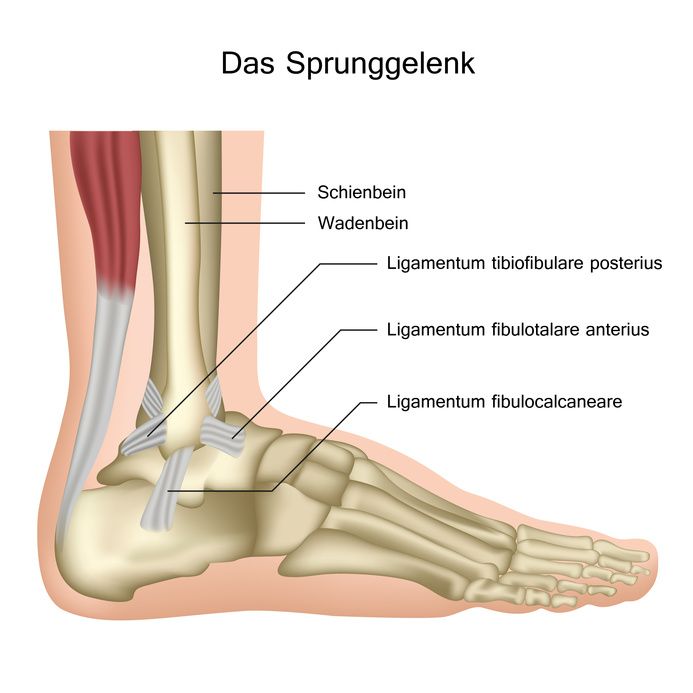
Anatomy of the ankle joint © bilderzwerg / Fotolia
Ankle osteoarthritis destroys the joint cartilage. The most common cause is a prior injury (trauma). Less frequently, ankle osteoarthritis develops as a consequence of another orthopedic condition such as arthritis.
Older individuals are more frequently affected by joint degeneration in the ankle, but younger people, especially active athletes, can also develop the condition.
A torn ligament often leads to chronic instability of the ankle joint. Over time, this instability can cause cartilage wear and eventually result in osteoarthritis of the ankle.
Injuries to the ankle can also result in fractures of the medial malleolus or lower fibula. Sometimes both the medial and lateral malleoli are fractured, often accompanied by cartilage damage.
High-impact sports and excess body weight can also significantly challenge the resilience of ankle cartilage.
Typical signs of an ankle fracture include
- a swollen, painful ankle with bruising (hematoma), and
- restricted mobility.
In Germany, professional associations report around 10,000 ankle fractures each year.
Malalignments are often responsible for increased stress on the ankle cartilage. Such malalignments may also occur after fractures, leading to premature cartilage wear and, ultimately, ankle osteoarthritis.
The so-called primary ankle osteoarthritis is much less common than secondary ankle osteoarthritis. It does not result from prior injury or disease but develops without a clear cause. A genetically determined insufficient cartilage structure is suspected. Compared to hip or knee osteoarthritis, primary ankle osteoarthritis is rare, as ankle cartilage has a unique biochemical composition and significantly greater resistance to pressure.
The stages of ankle osteoarthritis range from initial cartilage damage with mild pain to advanced forms with marked restriction of motion and persistent symptoms.
Extensive cartilage damage in the ankle due to advanced osteoarthritis results in a painful restriction of movement. Every step is painful. In later stages, pain may also occur at rest, significantly reducing the patient’s quality of life. Weight-bearing can cause swelling and inflammation, leading to severe ankle pain as the disease progresses.
Malalignments and sometimes ligament instabilities are also common. X-ray and MRI scans reveal joint destruction with narrowing or obliteration of the joint space and bony outgrowths that attempt to stabilize the joint. These findings may make surgery necessary.

The ankle joint is essential for walking © decade3d / Fotolia
In the early stages of ankle osteoarthritis, an arthroscopy can help slow disease progression. During this procedure, bony spurs on the tibia are removed to improve mobility and reduce pain. As osteoarthritis progresses, pain and restriction of motion in the foot and ankle worsen significantly. In severe cases, this can even affect the degree of disability.
Initially, targeted pain therapy is often used, for example with medication, physical therapy, or injections. If these measures are no longer sufficient, surgical treatments such as ankle fusion (arthrodesis) or ankle replacement (endoprosthesis) are available. Both aim to reduce pain and sustainably improve the patient’s quality of life.
Ankle Fusion for Ankle Osteoarthritis
Ankle fusion surgery (arthrodesis) significantly reduces pain in most patients. Alongside prosthetic replacement, ankle fusion is considered the treatment of choice and is widely performed in clinics.
The video shows the procedure of arthroscopic ankle fusion:
The technique of ankle arthrodesis has been refined in recent years. Cartilage remnants and diseased bone layers are removed.
The tibia and talus are internally stabilized with screws and/or an angular-stable plate, healing together in a process similar to fracture healing. Malalignments are corrected by removing bone wedges of defined size, allowing the foot to be properly aligned on the ground.
Most patients adapt well to ankle fusion. It enables walking smoothly and inconspicuously without special orthopedic footwear.
Ankle Replacement for Ankle Osteoarthritis
Although arthrodesis is still considered the gold standard in many clinics, an ankle replacement may be the better option when:
- both ankle joints are affected, or
- the patient wishes to preserve mobility as much as possible.
The prosthesis prevents overloading of neighboring foot joints and helps protect them from secondary osteoarthritis.
Patients with inflammatory polyarthritis particularly benefit from ankle replacement. They usually have a history of multiple surgeries on the lower extremities. For them, an ankle prosthesis preserves overall mobility and improves gait.
Therefore, ankle replacement offers significant advantages over arthrodesis, especially in cases of inflammatory joint destruction.
Depending on design, ankle prostheses are classified into
- uniaxial prostheses,
- semi-constrained two-component prostheses (hinge principle),
- multi-axial two-component prostheses (“ball-and-socket principle”), and
- three-component prostheses.
Three-component prostheses with mobile or fixed polyethylene inserts replace
- either only the central joint section between tibia and talus, or
- also the inner and outer talar shoulders.
The metal components are specially coated to promote bone ingrowth, eliminating the need for cement fixation. Due to advanced design, today’s systems produce only minimal wear, significantly reducing the risk of loosening and revision surgery.
Which Ankle Prosthesis Provides the Best Pain Relief and Mobility?
The talocrural joint allows not only hinge-like motion but also various complex movements around multiple shifting axes:
- gliding,
- slight inversion and eversion, and
- rotation.
Uniaxial two-component hinge prostheses therefore showed high loosening rates. Multi-axial two-component prostheses often lacked sufficient joint stability.
The modern three-component prostheses imitate the physiological movement axes much more effectively. Follow-up studies show they achieve significantly better results than older two-component models, with lower complication and loosening rates and greater restored mobility.
The cementless implantation of three-component prostheses also has advantages in case of explantation (removal of the prosthesis, e.g., if it loosens). Compared to older systems, less bone is lost during removal, making revision surgery or fusion safer.
Biomechanical studies show that three-component prostheses provide normal rotational and tilting stability. They currently best reproduce physiological ankle motion, as confirmed by pressure and force measurements during walking.
Thus, three-component ankle prostheses represent an excellent treatment concept for ankle osteoarthritis.























